A Multisensory Literacy Approach to Biomedical Healthcare Technologies: Aural, Tactile, and Visual Layered Health Literacies
by Kristin Marie Bivens, Lora Arduser, Candice A. Welhausen, & Michael J. Faris
Visual Health Literacies: I See Flu Near You
Candice A. Welhausen
Seasonal Flu and Risk Perception
Microscopic image of flu viruses. Seasonal flu varies in severity every year because different influenza viruses circulate. (photograph by F. A. Murphy, 2015, in the public domain)
Think about the last time you had flu-like symptoms. How did you feel? Did you have
a fever?
a headache?
a sore throat?
congestion?
body aches?
If you had one or more of these symptoms, you may have felt ill enough to stay home for a day or two, perhaps longer, and you may have been run down for a week or so thereafter. But chances are, if you're a healthy adult between the ages of about 18 and 65, you easily made a full recovery. Indeed, most healthy people tend to not be overly concerned about getting the flu. Rather, they perceive the illness as "a minor nuisance," as Peter Sandman and Jody Lanard (2005, p. 4) put it, because they usually do not become severely ill and/or experience life-threatening consequences.
From a public health perspective, however, the virus continues to pose a major health threat. In the United States, for instance, the Centers for Disease Control and Prevention (CDC, 2016c) estimated that "millions of people are sickened, hundreds of thousands are hospitalized[,] and thousands or tens of thousands of people die from flu every year."
The annual flu season generally runs from October to May (CDC, 2016c), and educational materials, particularly those that promote the flu shot, are usually disseminated in the fall and early winter because it takes a couple of weeks for the vaccine to become effective. For instance, the Facebook page for the University of Delaware's (UD) Healthy HENS (2015), a program affiliated with the university's Student Health Service, showed a status update posted in December during the 2015–16 flu season reminding students to get vaccinated.
Screenshot of flyer posted on the Healthy HENS (2015) Facebook page on December 11, 2015 advertising "Flu Shot Fridays"
Such health-related information is often communicated using visuals as the "Flu Shot Fridays" flyer demonstrates through its frowning sun, green "sick" face, and grimacing, yellow-green virus in the lower left-hand corner. Most public, non-expert audiences in the United States who might see this flyer (UD students, faculty, staff, and community members, for instance) are likely to easily understand how these visuals contribute to the flyer’s overall message because they are proficient in the visual literacies needed to understand this aspect of the overall message.
Indeed, visual literacy—the ability to interpret, construct meaning from, and produce visual forms—has long played a central role in art and design-related fields (e.g., Arnheim, 1969; Dondis, 1974; Elkins, 2009; Kress & van Leeuwen, 2006; Messaris, 1994). Over the past few decades, recognition of the importance of visual communication has also proliferated to other disciplines, reflecting what W. J. T. Mitchell (1994) has described as a "pictorial turn" (p. 11). This shift also lends insight into why non-expert readers can often easily understand and process health-related information conveyed visually, such as the illustrations in the "Flu Shot Fridays" flyer.
At the same time, research on visual literacies among non-experts tends to position visuals as supplementary to textual content, touted as a strategy for improving readers' comprehension (Osborne, 2006), and for communicating with audiences who are less proficient in alphabetic literacies (e.g., Houts, Doak, Doak, & Loscalzo, 2006) as well as culturally diverse groups (Kreuter, Lukwago, Bucholtz, Clark, & Sanders-Thompson, 2002).
In this section, I explore the ways that non-experts' visual literacy practices are both enabled and constrained by how health and disease are viewed in Western cultures by theorizing the visual conventions used in the mapping features of a crowdsourced flu-tracking program called Flu Near You (FNY): www.flunearyou.org. By viewing FNY's maps to better understand if seasonal flu is spreading in their area, public audiences engage in a range of visual literacy practices that they may then use to make health-related decisions related to flu prevention like deciding whether to get the flu shot and/or to sanitize their hands more frequently when flu is spreading.
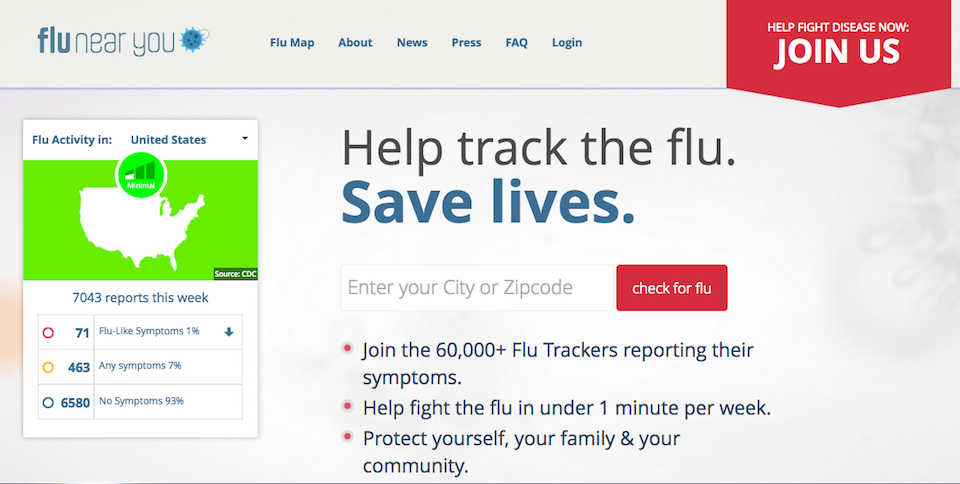
Screenshot of FNY home page (image taken July, 2016; used with permission)
FNY and Digital Participatory Flu-Tracking
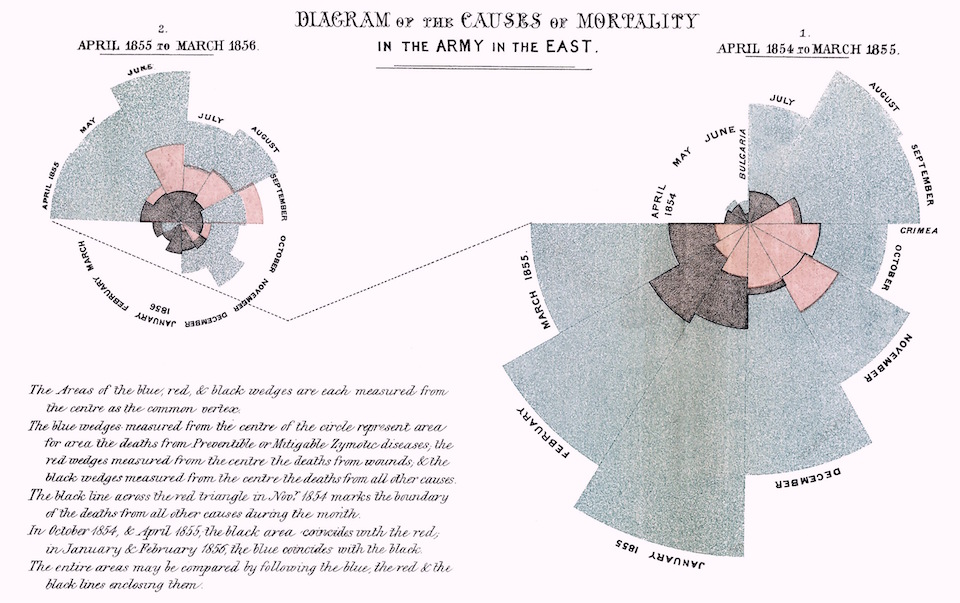
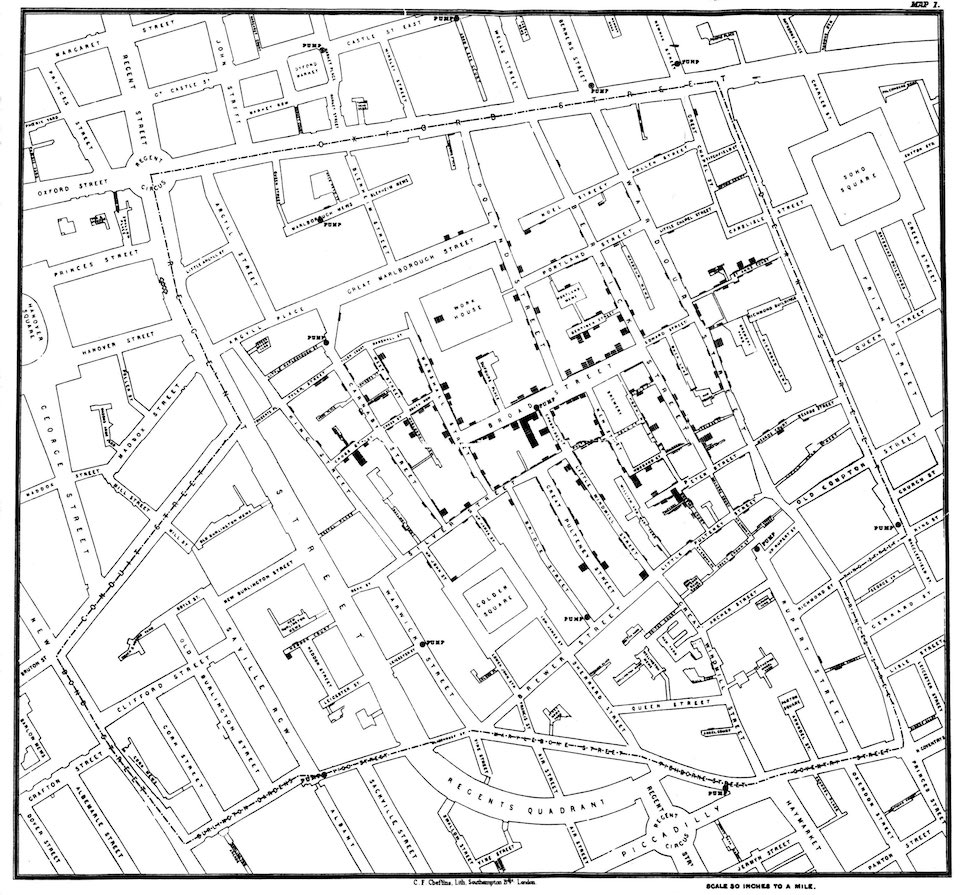
Historically, visual quantitative information about the spread of infectious and communicable diseases was usually created by early public health researchers who used this information to advance particular kinds of public health arguments (e.g., Florence Nightingale's [1858] rose diagrams and John Snow's [1854] map of a cholera outbreak).
Nightingale's (1858, in public domain) diagrams compared mortality rates in the English city of Manchester to those for British soldiers during the Crimean war, which she created to advance her argument for sanitary reform in hospitals (see also Brasseur, 2005).
John Snow's (1854, in public domain) "Broad Street" map documents a severe cholera outbreak that occurred in London’s Golden Square neighborhood in late August of 1854 (see Brody, Vinten-Johansen, Paneth, & Rip, 1999).
In the twenty-first century, however, participatory flu-tracking programs like Influenzanet.eu (Europe), FluTracking.net (Australia), and FluNearYou.org (United States, Puerto Rico, and Canada) have arguably blurred the role of expert and non-expert, allowing public audiences to not only contribute to user-contributed data collection but to also visualize this information.
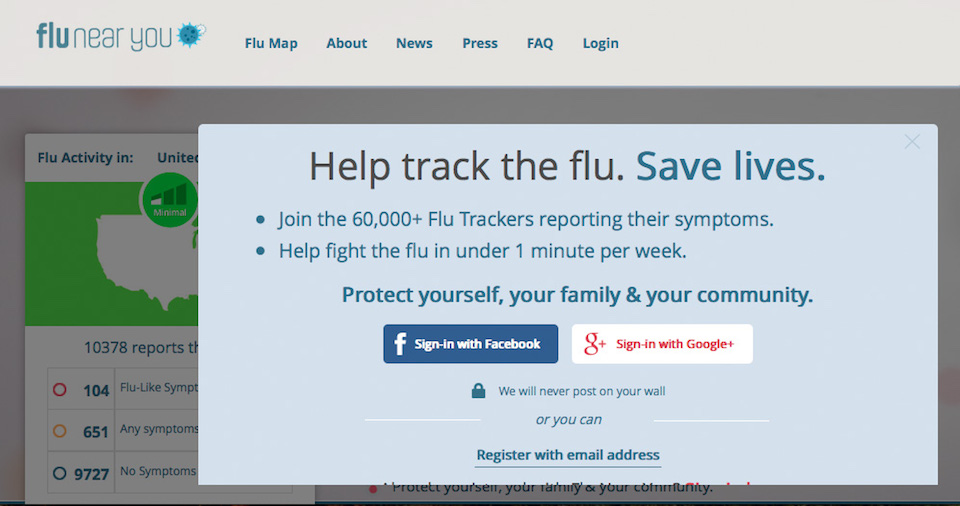
FNY is a participatory flu-tracking system that premiered in November 2011 and was designed by a team of public health researchers and information technology professionals to collect voluntary information about flu symptoms from the public in the United States, Puerto Rico, and Canada. In March of 2015 the program reported 140,000 registered users (Smolinski et al., 2015), while as of June 2016 the splash page on the program's website suggested that 60,000+ registered users were participating.
Screenshot of FNY Splash Screen (image taken July, 2016; used with permission)
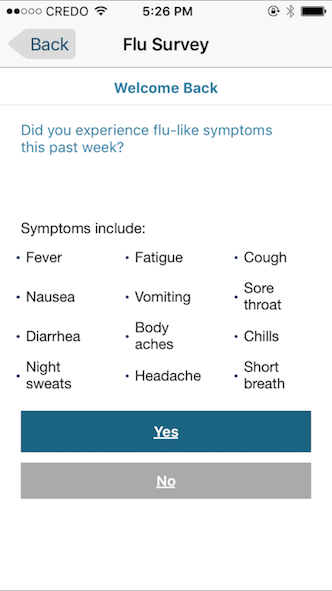
Participants register by providing an e-mail address and demographic information: gender, birth month and year, and zip code. They then receive weekly e-mails and/or smartphone notifications via the program's mobile app prompting them to choose flu-related symptoms from a list (e.g., sore throat, fever, cough) that they and/or their family members (if they register members of their household) may have experienced in the preceding week.
Screenshot of the weekly participant report from FNY's website (image taken July, 2016; used with permission). On February 25, 2016 FNY notified registered users via e-mail that the website (but not the mobile app) would now also track symptoms associated with several mosquito-transmitted illnesses: Zika, Chikungunya, and Dengue fever.
Screenshot of the weekly participant report from the FNY mobile app (image taken January, 2016; used with permission)
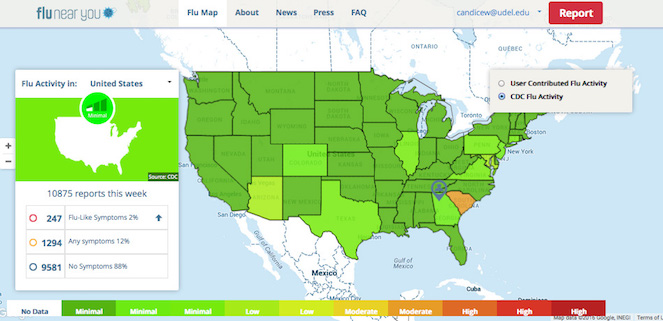
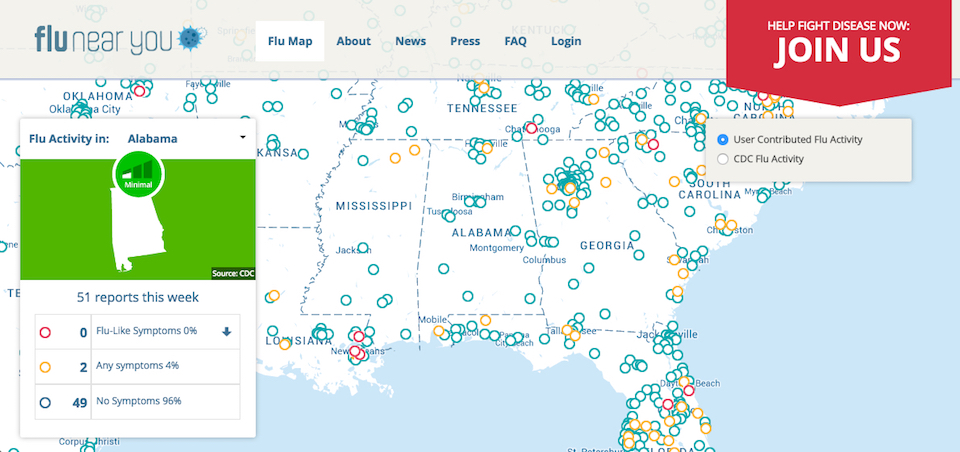
Registered users (and visitors to the site) can access two types of maps that show flu activity: a map of the continental United States showing CDC-generated flu activity collected through traditional flu-tracking methods, and a map of the same geographic region showing user-contributed flu activity.
Screenshot of CDC-generated flu activity from the FNY website (image taken July, 2016; used with permission)
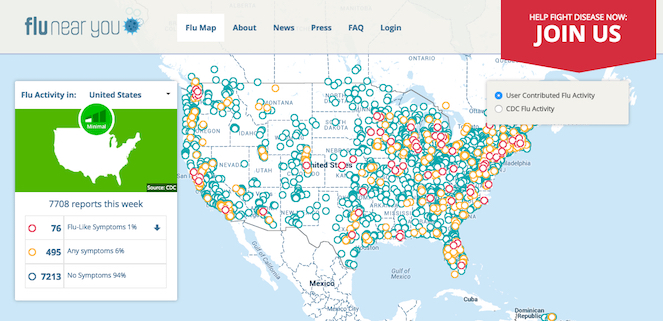
Screenshot of user-contributed flu activity from the FNY website (image taken July, 2016; used with permission)
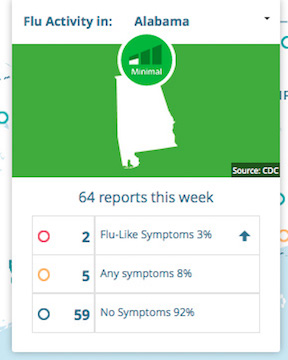
In the user-contributed flu activity map, viewers can see activity for individual states on the FNY website by clicking on the state of interest in the drop-down menu (included in the map’s legend on the left side of the screen).
The map's legend on the program's website also includes the total number of user-contributed reports nationally and by state (when viewers use the drop-down menu to select a state) and the number of these reports that include "flu-like symptoms" (red circle), "any symptoms" that may be associated with the flu (orange circle), and "no symptoms" (blue circle).
Screenshot of user-contributed flu activity by state from the FNY website (image taken July, 2016; used with permission)
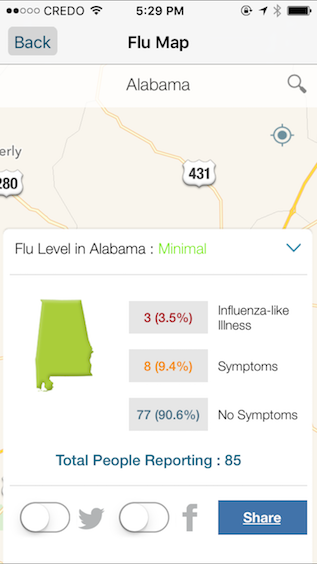
Mobile app users can also view user-contributed information at the state and/or city level.
Screenshot of user-contributed flu activity by state from FNY mobile app (image taken January, 2016; used with permission)
Screenshot of user-contributed flu activity by state: city/town level detail from the FNY mobile app (image taken January, 2016; used with permission)
Exact numbers are not given on the CDC-generated map. Rather this map categorizes aggregate flu activity using the categories shown on the legend below.
Legend of color coding system on CDC flu activity map (image taken July, 2016; used with permission)
Benefits of Participatory Flu-Tracking
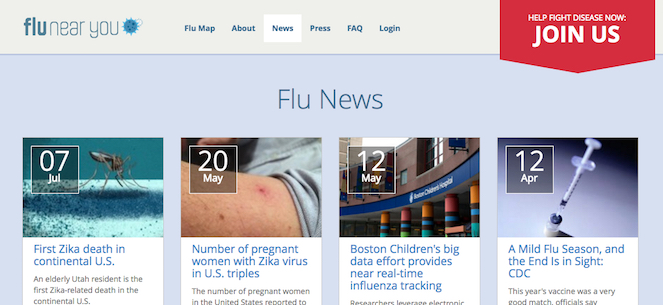
Like its predecessors Influenzanet.eu and FluTracking.net, which track user-reported flu activity in Europe and Australia, respectively (see Wójcik, Brownstein, Chunara, & Johansson, 2014), FNY can potentially enhance the data about flu that public health agencies collect by gathering select health-related information directly from public audiences (Smolinski et al., 2015). It is important to note that such participatory programs do not replace traditional flu-tracking methods such as those used by CDC. Rather, such participatory information is potentially useful from a public health perspective, providing information that researchers might use to promote behaviors like getting the vaccine that reduce flu incidence in the population. However, the FNY website and mobile app were designed for non-experts. Thus, many of the program's features—links to news stories about the flu and other infectious and communicable diseases, the vaccine finder tool, and the program's maps—attempt to appeal specifically to this audience.
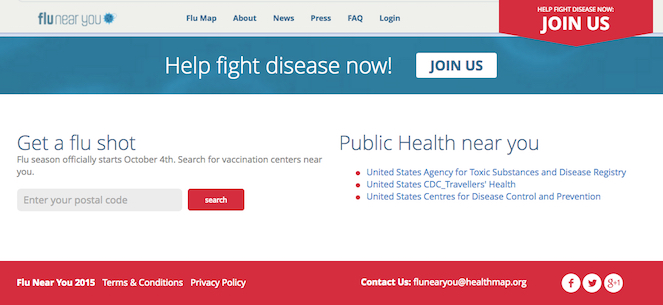
Screenshot of "Flu News" section on the FNY homepage (image taken July, 2016; used with permission)
Screenshot of the "vaccine finder" tool on the FNY homepage (image taken July, 2016; used with permission)
Of these resources, however, arguably the maps that show user-contributed flu activity provide the most consistently useful information for the program's non-expert users for several reasons. Flu News, the vaccine finder tool, and the CDC-generated flu activity map can easily be found on other websites. Further, once users have been vaccinated (or have decided to not get vaccinated), the vaccine finder tool is no longer likely to be useful until the next flu season. FNY participants may also be more likely to get the vaccine, particularly early in the season, because presumably these users already have a higher interest in tracking flu (and thus may be more likely to engage in prevention behaviors). Additionally, the program prompts participants to report if they have received the vaccine every week until the user answers "yes," further increasing the likelihood that participants will acquiesce and get the shot, potentially rendering this tool irrelevant early in the flu season.
The user-generated maps are also the only feature that is unique to the program, providing detailed information about how the flu is spreading in real time in viewers' specific locations. The most compelling reasons that FNY users may decide to participate then include
contributing to data collection (and helping researchers who manage the program potentially track flu); and
being able to visualize data contributed by all users (the user-generated maps) so they can use these maps to help them decide what flu prevention behaviors (e.g., getting the flu shot, sanitizing hands more frequently, avoiding contact with others, limiting travel) they may engage in, if any, throughout the flu season.
FNY's Mapping Feature: Visual Literacy Practices
Many of the design strategies that are commonly used in contemporary data visualizations adhere to visual conventions that became established in the nineteenth century (Friendly, 2008). Further, viewers in the United States often understand how to interpret these forms because they are already familiar with the visual conventions and design strategies that these graphics use (see Kostelnick, 2004; see also Kostelnick & Hassett, 2003).
Consequently, many FNY users may already have many of the requisite visual literacies needed to understand the program's disease maps. Indeed, with the exception of the About page, which states that the user-generated maps show users "when the flu is around," the legend on both of the maps showing the number of reports by each category, and the color-coding system at the bottom of the CDC map, no additional visual or written instructions are provided on the site or in the mobile app that explain to viewers how to read the maps.
Example legend for map of user-contributed flu activity from the FNY mobile app (image taken January, 2016; used with permission)
Arguably, the purpose of the legend for the user-generated maps is to provide detailed numeric information about the reports (e.g., percentage of users reporting "flu-like," "any," or "no symptoms") detailing state-level information, but not necessarily to explain the map's color coding system, which follows the convention of using warmer colors to show cases and/or increasing incidence (red and yellow in FNY's maps). The CDC map also follows this convention by using warm colors to indicate higher levels of flu activity (i.e., dark red indicates the highest level of flu incidence, while green indicates the lowest level).
Yet the legend under the CDC map as well as the brief explanation on the program's About page (shown below) may be unnecessary for many readers. FNY users probably know (through previous exposure to such visuals) how to read the color scheme in both maps, and they probably also know the rhetorical purpose of a thematic map—in this case, to visually situate flu incidence in time and space.
Indeed, the design of FNY's maps—both the user-contributed flu activity and CDC-flu activity—draws on visual conventions that are well-established for this particular graphical genre. Thus, because viewers are likely to be literate in this form of visual communication, they potentially have the skills to engage in a fuller range of visual literacy practices in order to make health-related decisions like deciding whether to engage in flu prevention behaviors such as getting the flu shot or sanitizing hands more frequently during high levels of flu activity reported via the maps.
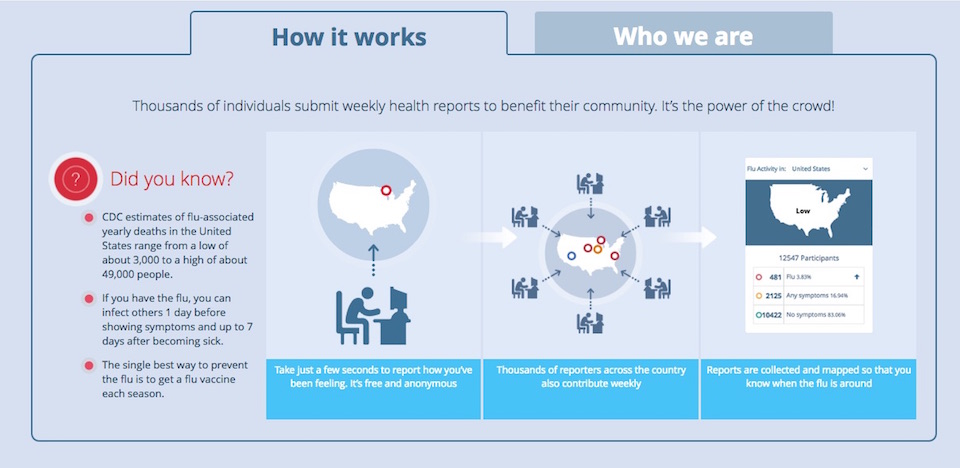
Screenshot of FNY's "About" page's "How It Works" tab (image taken July, 2016; used with permission)
Further and importantly, FNY's maps can be useful to non-experts throughout the flu season because such visual information can guide them in determining how their risk of contracting the flu may be changing. Educational materials like the Healthy HENS's (2015) "Flu Shot Fridays" flyer shown earlier are usually disseminated towards the beginning of the annual flu season (before flu activity has peaked) and consequently position getting the flu shot (a specific, one-time preventative behavior) as particularly important during this time frame.
Indeed, the CDC (2016a) recommended getting vaccinated, which they state is the most effective prevention strategy, at the beginning of the flu season well before the flu is beginning to spread. However, the full season runs for approximately eight months with peak activity frequently occurring sometime between December and February (CDC, 2016d). Thus while people may be more likely to get the flu during these months, one can get the flu any time flu viruses are spreading.
Each flu season is also different. Some flu viruses may be more prevalent than others in a particular year, which means that the vaccine's efficacy also varies from year to year. Consequently researchers do not know how effective each year's vaccine was until the end of the season, meaning that even if someone gets the flu shot during the recommended timeframe, she may still become infected.
These factors demonstrate that flu risk is not static but rather can change dramatically not just during one flu season but across different flu seasons. FNY's maps then can be particularly useful not just for viewers who have not been vaccinated by showing when flu activity is increasing but for viewers who have been vaccinated because getting the vaccine does not necessarily ensure protection. The vaccine's efficacy is between 50–60% when it protects against the flu viruses that are spreading during a given year (CDC, 2016e). Consequently getting vaccinated each year can substantially mitigate the risk of getting sick. But it might also give those who get vaccinated a false sense of security as well as cause them to become more lax about engaging in other flu prevention behaviors like sanitizing hands more frequently and avoiding close contact with other people.
Both types of maps in FNY's program—CDC-generated and user-contributed—can then signal to viewers when they may want to engage in these other preventative practices. More specifically, the CDC map shows flu incidence across the continental United States, which allows viewers to determine if flu activity is increasing overall in their state of residence or in any state of interest. However, the maps showing user-contributed information—particularly on the mobile app, which provide location-specific detail from other contributors—might be much more relevant for viewers. Indeed these maps do much more than just show viewers "when the flu is around," as the About page explains; they show users where "the flu is around" each week in real time as the user-contributed maps are updated when participants submit a flu report. Viewers can then use this mapping tool to assess flu risk across the flu season and decrease or increase flu prevention behaviors like sanitizing hands more frequently and avoiding close contact with other people as their risk changes each week.
Controlling Flu Risk and the Biomedical Model
FNY's mapping features allow non-expert users to engage in visual literacy practices related to assessing their potential exposure to flu, which can subsequently enable them to make decisions about engaging in flu prevention behaviors. However, using these visuals to assess flu risk can also give viewers an illusory sense of control over their potential exposure, aligning with a Western perspective towards disease and health.
Like all disease maps, FNY's maps situate a particular disease—in this case flu—in both time and space, positioning the disease as an external entity. The maps showing user-contributed information accomplish this by using circles to pinpoint the exact places where flu (red), "any symptoms" (yellow), and "no symptoms" (blue) are occurring. This visual choice disassociates flu from bodily experience, invoking a separation between the viruses that cause the illness and the physical experience of having the flu. Seasonal flu can be caused by a number of influenza viruses, which exist as independent organisms that do infect individual bodies. However, this artificial separation between the disease and the embodied experience of the disease, which is enacted visually in all disease maps, allows us to view flu viruses as "deviation from normal biological functioning," as Elliot Mishler (1981, p. 3) put it in his discussion of the ideologies that underlie Western medicine.
Flu is then understood as an "other" that can and should be controlled. Further, in order to control the spread of an infectious and/or communicable disease like flu, the causal agent needs to also be consistently identifiable, reflecting the "doctrine of specific etiology" (Mishler, 1981, p. 3). Flu complicates this perspective, however, because there are many influenza viruses, some of which can be particularly virulent like the pandemic strain of "Spanish" flu that struck during the 1918–19 flu season, killing an estimated 50 million people (Johnson & Mueller, 2002). Thus visually positioning flu as a uniform other in a disease map may give the illusion that a more definitive sense of control can be established over the spread of flu than may actually be possible.
These two points also tie into "the universality of a disease taxonomy" (Mishler, 1981, p. 3), which is the notion that "disease symptoms and processes are expected to be the same in different historical periods and in different cultures and societies" (p. 9). This ideology plays out in both the user-contributed and the CDC-generated flu activity maps through their color-coding schemes. In the CDC map, for instance, quantitative information about flu incidence is flattened into three main categories: low (green shades), medium (yellow and orange shades), and high (red shades). Color choice and shading indicate the level of flu activity, but there is no further nuanced information. Rather, each category promotes flu as uniformly "low" or "medium" or "high" throughout the space shown. In other words, all areas with "low" flu activity or "high" flu activity are visually the same regardless of how that activity may be fluctuating within the space as well as how virulent the flu strains may be that are infecting people in the area.
As in all disease maps, color creates a visual taxonomy by giving the illusion of consistency. In the CDC-generated maps, any number of viral strains with varying degrees of potency could be potentially circulating in the areas shown. More specifically, while an area might visually indicate "high" flu activity (red), such activity might be from viral strains that are relatively mild, while the inverse may also be true. For instance, a novel, virulent pandemic strain may be emerging in an area that is (at the time the map was created) coded green because the threat has not yet been identified. The maps created with user-contributed data, too, use a similar classification scheme to organize flu activity into absolute categories—flu (red), "any symptoms" (yellow), "no symptoms" (blue)—with no additional information to qualify the potential severity.
These visual strategies, which are now often conventional in disease maps, advance a proposition about how a particular disease is affecting a particular space at a particular moment in time. Indeed, if a FNY user glances at the mobile app and sees a lot of other users reporting flu-like symptoms in her area, she will probably perceive that her risk of getting the flu is increasing and vice versa. That is, she may interpret many user reports of no symptoms as no flu risk. Yet as human populations have become increasingly mobile, a person's location is often not fixed. Indeed it is not uncommon for people to live, work, and vacation in different geographic regions, disrupting the notion that location-based information about the spread of infectious and communicable diseases is always useful for assessing risk.
Disease maps are frequently used to communicate visual risk information to non-experts. For instance, in March and April of 2016 information about the spread of Zika, a mosquito-borne virus that can cause severe neurological conditions, was frequently communicated to non-experts by mainstream news media using maps showing the current and potential range of the mosquitoes that transmit the virus (Welhausen, forthcoming). These maps—like FNY's maps and all other disease maps—provide selective information, tied to a fixed representation of reality about how the spread of a particular disease exists temporally and spatially, which often gives the illusion of control over that risk.